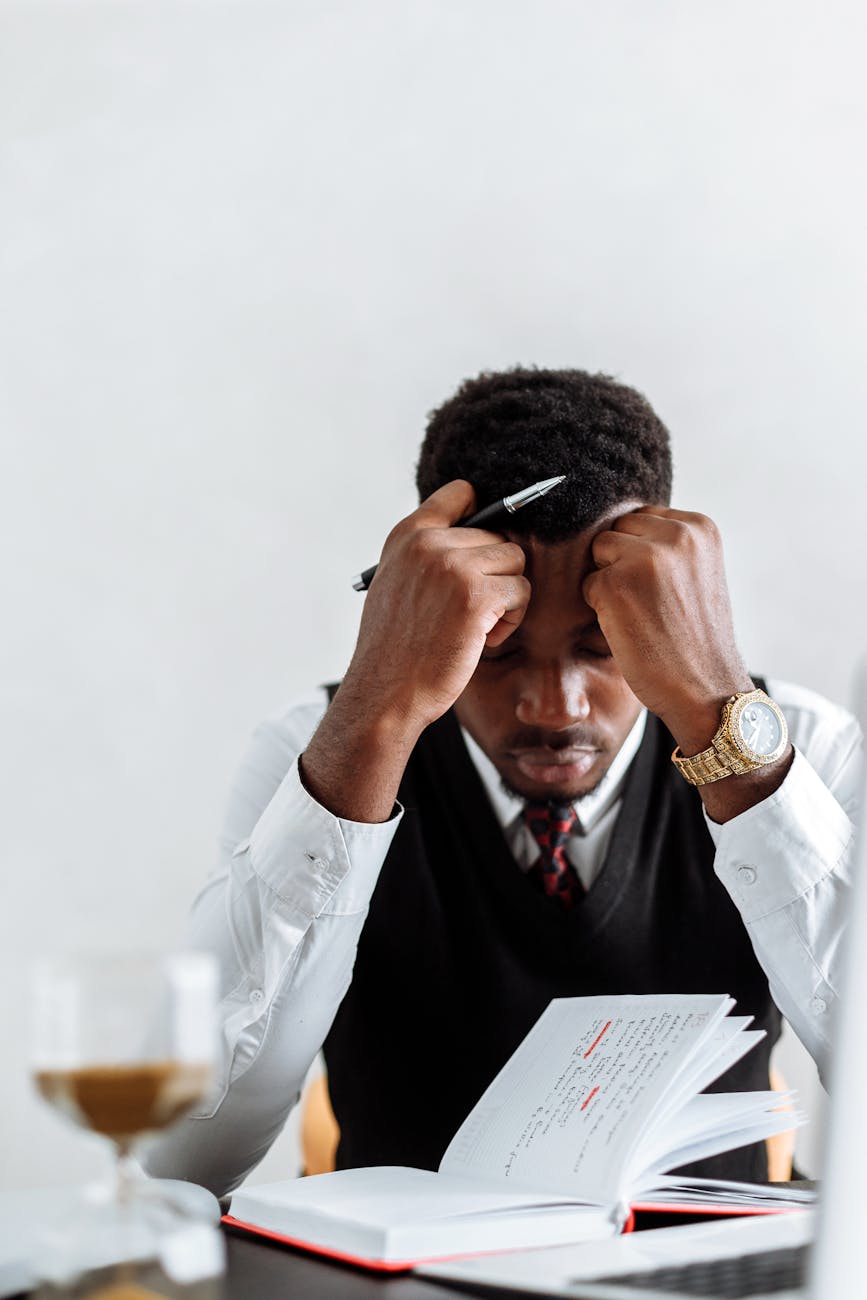

Interacting with a narcissist is often psychologically draining and spiritually destabilizing. Narcissists thrive on power dynamics, emotional control, and the manipulation of perception. Understanding how to identify them—and why confrontation can be dangerous—is essential for protecting one’s mental, emotional, and spiritual well-being. Though narcissists may appear charming, confident, and persuasive, their underlying motives often revolve around dominance, validation, and control.
At first, narcissists are magnetic. They exude charisma, attentiveness, and apparent empathy, drawing others in with flattery and idealization. This initial phase, known as love bombing, creates emotional dependency by making the target feel uniquely valued (Campbell & Miller, 2011). However, this admiration is conditional—it exists only as long as the narcissist gains something in return. Once the novelty fades or control is established, they shift to devaluation, criticism, or silent withdrawal, leaving the victim confused and emotionally destabilized.
Spotting a narcissist requires recognizing the patterns beneath their charm. One of the earliest signs is an inflated sense of self-importance. Narcissists subtly center conversations around themselves, exaggerate achievements, and display contempt for perceived inferiority (APA, 2022). Their language often includes grandiose claims of superiority or uniqueness, paired with an absence of genuine curiosity about others. This imbalance of focus serves as an early red flag.
Another key indicator is the absence of empathy. While narcissists can mimic empathy cognitively, their compassion lacks emotional depth. When others express pain or vulnerability, narcissists may respond with impatience, dismissiveness, or strategic sympathy meant to preserve their image. This “selective empathy” enables them to maintain control over others’ emotional states without genuine concern (Wai & Tiliopoulos, 2012). Over time, this emotional void becomes increasingly evident.
Narcissists are also experts in projection—accusing others of the very faults they themselves possess. When confronted with their own flaws, they deflect blame, reverse roles, and create confusion. This psychological manipulation, often termed gaslighting, distorts reality and erodes the victim’s sense of self-trust (Stern, 2018). Victims begin questioning their memory, judgment, and worth, which deepens their dependency on the narcissist for validation.
Importantly, calling out a narcissist rarely leads to resolution. In fact, it often provokes narcissistic rage—an explosive reaction to perceived criticism or humiliation (Kohut, 1977). Because narcissists rely on grandiose self-images to survive psychologically, any challenge to their ego triggers intense defensiveness. They may retaliate with verbal attacks, character assassination, or emotional withdrawal. Thus, confronting them directly can escalate conflict rather than foster accountability.
The danger of confrontation lies in misunderstanding the narcissist’s psychology. Unlike emotionally healthy individuals who can process feedback, narcissists interpret criticism as a personal attack. Their fragile ego cannot tolerate exposure. As a result, attempts to hold them accountable often lead to increased manipulation or punishment. The safest strategy is not confrontation but detachment—removing oneself emotionally and physically from their sphere of control (Ronningstam, 2016).
Another subtle sign of narcissism is the constant need for admiration. Narcissists crave praise and attention, not out of confidence but from an inner void. Their validation must be external, and they often manipulate situations to ensure the spotlight remains on them. When admiration wanes, they experience emptiness and frustration. This dependency creates cycles of idealization and devaluation in relationships, leaving others emotionally exhausted.
Spiritually, narcissists often disguise their motives under moral or religious language. They may quote scripture, speak of divine calling, or emphasize their “good works” to appear righteous. Yet, their fruits betray them. As Christ warned, “Ye shall know them by their fruits” (Matthew 7:16, KJV). The fruits of narcissism—pride, deceit, manipulation, and division—reveal the truth behind the mask of holiness. Such individuals often twist spirituality into a tool for self-worship.
Narcissists also lack genuine accountability. They will offer apologies without change, often using remorse as a manipulation tactic rather than a step toward repentance. Their apologies are typically vague (“I’m sorry you feel that way”) or conditional (“If you hadn’t done that, I wouldn’t have reacted”). True accountability threatens their self-image, so they feign contrition to maintain control (Miller & Campbell, 2008).
In social settings, narcissists often engage in triangulation—pitting individuals against each other to maintain dominance. They subtly spread misinformation, compare people, or create competition for their approval. This tactic keeps others off balance and prevents unity. Triangulation ensures the narcissist remains at the center of attention and power, much like a puppet master orchestrating invisible strings (Ward, 2011).
Another telltale sign is their pattern of boundary violation. Narcissists test limits early, dismissing others’ comfort zones as unnecessary or “overly sensitive.” They may intrude on personal space, privacy, or autonomy while justifying it as intimacy or honesty. Boundaries threaten their control, so they often ridicule those who set them. Over time, this erodes self-respect in the victim and reinforces dependency.
One of the most effective tools against narcissistic manipulation is gray rocking—a technique that involves emotional neutrality. By refusing to react with emotion or attention, the target becomes uninteresting to the narcissist. Since narcissists thrive on reaction and drama, indifference starves their ego of fuel. However, even this must be done cautiously, as overt withdrawal can provoke retaliation if they sense loss of control.
Psychologically, narcissists operate from deep insecurity masked by superiority. The roots of narcissism often lie in childhood trauma, inconsistent affection, or overvaluation by caregivers (Kernberg, 1975). Their grandiosity compensates for buried shame and fear of inadequacy. Recognizing this internal fragility can help survivors detach without personalizing the abuse, understanding that the narcissist’s cruelty reflects self-hatred projected outward.
Biblically, narcissistic behavior aligns with the archetype of Lucifer—once radiant and favored, yet corrupted by pride and self-exaltation. Isaiah 14:12–14 (KJV) describes this fall vividly: “For thou hast said in thine heart, I will ascend into heaven… I will be like the Most High.” Narcissists, too, crave admiration and dominance, rejecting humility and accountability. This spiritual parallel underscores the moral gravity of unchecked ego.
In romantic relationships, narcissists exploit emotional intimacy as a power source. They may mirror their partner’s values and desires to create a false sense of connection. Once trust is established, they gradually dismantle it through criticism, neglect, or betrayal. The cycle of idealization and devaluation can lead to trauma bonding, where the victim feels addicted to the relationship despite the abuse (Carnes, 2019).
When dealing with a narcissist, knowledge becomes protection. Rather than attempting to expose or fix them, the safest path is strategic disengagement. This may involve limiting communication, seeking professional support, and prioritizing emotional recovery. As Ronningstam (2005) notes, the narcissist’s change must originate from within, and external confrontation rarely catalyzes transformation. Self-preservation, not persuasion, must be the goal.
Spiritually, discernment is critical. Scripture instructs believers to “mark them which cause divisions and offenses contrary to the doctrine…and avoid them” (Romans 16:17, KJV). This counsel applies to narcissists who distort truth for self-gain. Wisdom involves recognizing the pattern, not debating the deceiver. Silence, distance, and prayer become tools of both self-protection and divine obedience.
Ultimately, dealing with a narcissist requires both psychological understanding and spiritual fortitude. They are masters of illusion, but truth dismantles their control. Recognizing their tactics—grandiosity, gaslighting, projection, manipulation, and charm—allows one to disengage strategically. Never calling them out is not cowardice; it is wisdom. The narcissist’s downfall often arrives not through confrontation, but through the quiet withdrawal of those who refuse to feed their ego.
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.).
Campbell, W. K., & Miller, J. D. (2011). The handbook of narcissism and narcissistic personality disorder: Theoretical approaches, empirical findings, and treatments. Wiley.
Carnes, P. (2019). The betrayal bond: Breaking free of exploitive relationships. Health Communications.
Kernberg, O. F. (1975). Borderline conditions and pathological narcissism. Jason Aronson.
Kohut, H. (1977). The restoration of the self. International Universities Press.
Miller, J. D., & Campbell, W. K. (2008). Comparing clinical and social-personality conceptualizations of narcissism. Journal of Personality, 76(3), 449–476.
Ronningstam, E. (2005). Identifying and understanding the narcissistic personality. Oxford University Press.
Ronningstam, E. (2016). Narcissistic personality disorder: A current review. Current Psychiatry Reports, 18(2), 9.
Stern, R. (2018). The gaslight effect: How to spot and survive the hidden manipulation others use to control your life. Harmony Books.
Wai, M., & Tiliopoulos, N. (2012). The affective and cognitive empathic nature of the dark triad of personality. Personality and Individual Differences, 52(7), 794–799.
Ward, T. (2011). The subtle power of spiritual abuse. Bethany House.